Malaria Detection
As recently as 2005, malaria prevalence exceeded 20% in many parts of Zanzibar. An increase in malaria prevention interventions, including universal coverage with insecticide-treated bed nets and indoor residual spraying (in 2007), have resulted in a dramatic decline in malaria prevalence in Zanzibar. However, the persistence of endemic malaria transmission in surrounding areas (Tanzania Mainland and Kenya) leaves Zanzibar vulnerable to sudden outbreaks and re-establishment of ongoing, perennial malaria transmission. Improved surveillance and epidemic response capacity are essential to maintain control, prevent the resurgence of the disease. Early epidemic detection systems are an essential way for timely detection of sudden increases in malaria transmission, and mobile health (mHealth) is an innovative way to combat malaria increases.
Active Case Detection
The Zanzibar Malaria Control Program (ZMCP), in collaboration with the President’s Malaria Initiative (PMI), the U.S. Centers for Disease Control and Prevention (CDC), and RTI International (RTI), developed and implemented the Malaria Epidemic Early Detection System (MEEDS). MEEDS Zanzibar relies on mobile-phone based reporting of malaria case reports and indicators from government primary health care units in Zanzibar. This real-time surveillance data allows ZMCP to make data-driven decisions regarding when and where to investigate sudden increases in transmission, initiate active case detection, and apply more comprehensive coverage of malaria interventions.
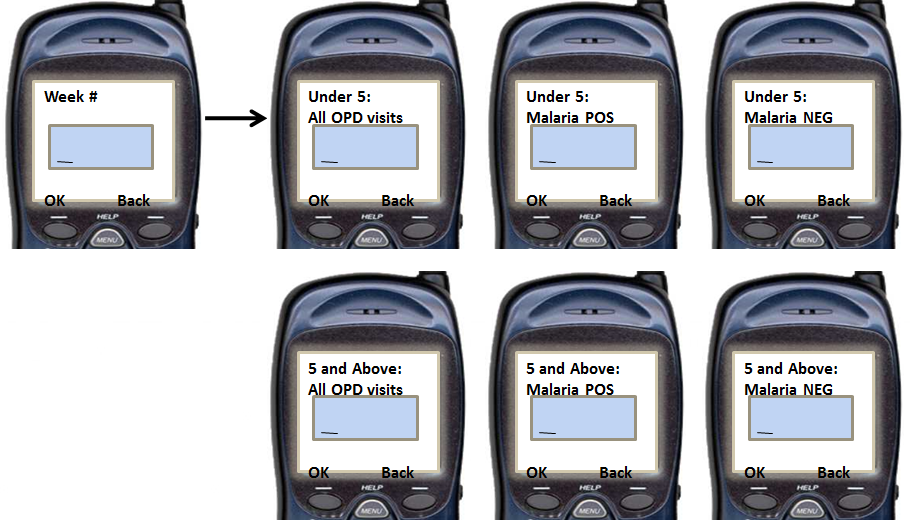
In 2008 MEEDS broke ground in mHealth systems by enabling facilities to report new malaria cases via simple feature phone handsets, and enabling the ZMCP to detect new epidemic outbreaks within two weeks of onset. With MEEDS, health facility officers in clinics use simple cell phone handsets to submit essential case data. The data are transmitted to a gateway via Unstructured Supplementary Service Data (USSD). The data are then stored on a remote server accessible through secure website for data management and analysis. The server and data relay are managed through SELCOM.
MEEDS was initially implemented at 10 health facilities in 2008 to transmit weekly aggregate case data. In late 2008, 42 more sites were added to the system. The number was increased again by 17 additional sites in early 2010 and by 21 more sites in late 2010. MEEDS is currently used by all public health facilities in Zanzibar
In 2013 ZMCP was renamed the Zanzibar Malaria Elimination Programme (ZAMEP) RTI has worked closely with the ZAMEP since 2008 to strengthen their ability to manage and make effective use of MEEDS. Support has included technical assistance with data analysis, hotspot mapping, management, and supervision.
Active Response
 Building on the success of MEEDS, the ZAMEP, in collaboration with the PMI, USAID, CDC, and RTI, have developed Coconut Surveillance. Coconut Surveillance enables district malaria officers to actively monitor and respond to new case reports received via MEEDS. MEEDS and Coconut Surveillance are helping Zanzibar to identify and treat many otherwise undiagnosed malaria cases, identify hot spots and transmission patterns, and respond rapidly to new outbreaks. These mHealth applications are helping Zanzibar to sustain the remarkable gains it has made against this dangerous and debilitating disease.
Building on the success of MEEDS, the ZAMEP, in collaboration with the PMI, USAID, CDC, and RTI, have developed Coconut Surveillance. Coconut Surveillance enables district malaria officers to actively monitor and respond to new case reports received via MEEDS. MEEDS and Coconut Surveillance are helping Zanzibar to identify and treat many otherwise undiagnosed malaria cases, identify hot spots and transmission patterns, and respond rapidly to new outbreaks. These mHealth applications are helping Zanzibar to sustain the remarkable gains it has made against this dangerous and debilitating disease.
From July-December 2012, health facilities in Zanzibar used MEEDS to report 980 new cases of malaria. District malaria officers using Coconut Surveillance responded actively to each new case, testing 3,228 household members, and identifying 223 previously unidentified malaria cases. ZMCP’s sustained campaign has reduced malaria incidence rates in Zanzibar significantly and has sustained this reduction. An aggressive location-based case response and management system, such as Coconut Surveillance, could potentially eliminate the disease.
- Login to post comments
- Printer-friendly version
 PDF version
PDF version