Zambia Electronic Perinatal Records System RTI Project #08330
Zambia Electronic Perinatal Records System
Final
Technical Report
(January to September 30, 2006)
Submitted to:
Dr. Robert Goldenberg, Principal Investigator
University of Alabama at Birmingham
Department of Obstetrics & Gynecology
619 South 19th Street, OHB 555
Birmingham, AL 35249-7333
Submitted by:
Eileen Reynolds
RTI International
3040 Cornwallis Road
P.O. Box 12194
Research Triangle Park, NC 27709-2194
November 3, 2006
Table of Contents
Exhibit 3: ARV care (Regimen given Today form) 9
Exhibit 4: Lab Results display 10
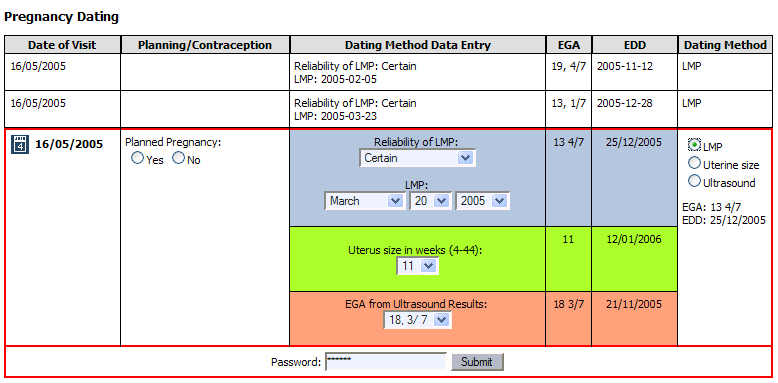
Exhibit 5: Pregnancy Dating 11
Exhibit 6: Delivery Summary 12
|
ART |
antiretroviral therapy |
|
CIDRZ |
Center for Infectious Disease Research in Zambia |
|
LUDHMT |
Lusaka Urban District Health Management Team |
|
PMTCT |
Preventing Mother-to-Child Transmission |
|
UAB |
University of Alabama at Birmingham |
|
UI |
user interface |
|
UTH |
University Teaching Hospital |
|
VCT |
Voluntary Counseling and Testing |
|
ZEPRS |
Zambia Electronic Perinatal Records System |
|
ARV |
Anti-Retroviral |
Dr Perry Killam, an American pediatrics physician in Lusaka, and Chris Kelley, an American software engineer in Cape Town, South Africa, are responsible for managing the deployment of ZEPRS in Lusaka. Dr. Killam and Mr. Kelley began their collaboration in January, 2006, about a month before the ZEPRS deployment started. Dr. Killam manages the clinical operations – monitoring how the clinicians interact with the applications, compiling change requests, and communicating and reviewing the change process with Mr. Kelley. Mr. Kelley, who wrote most of the ZEPRS application, manages and implements software updates. It has been a very productive working relationship. Mr. Kelley and Dr. Killam communicated almost daily about updates or bug fixes that were needed for the ZEPRS system. During this period, Dr. Killam worked with Lusaka clinicians in the deployment of ZEPRS to eleven clinics in Lusaka. Many of the changes to the system were in response to requests by clinicians or changes made to enhance a current process. To date (October 19 2006) over fourteen thousand patients have be tracked with the ZEPRS application since its debut February 2, 2006.
Most of the changes to the ZEPRS application have been routine – additions of items to dropdown menus or fields to forms. Bugs in the system were quickly identified and fixed – the most notable were a bug in EGA/ADD calculation and data errors on some of the new reports. Mr. Kelley installed new builds (updates) to the application almost every week. Mr. Kelley is able to install these updates on the Lusaka server using a secure connection over the Internet.
Some of the changes to ZEPRS are worth highlighting. These changes include the following items:
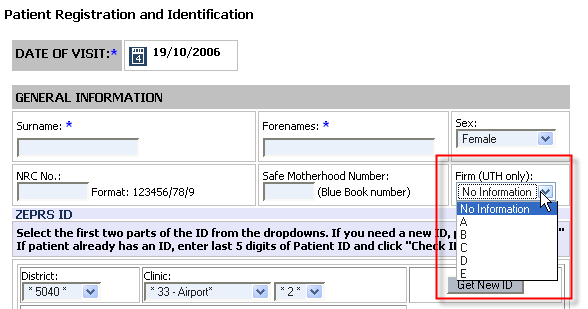
Demographics
Added “Firm” field to store what UTH Firm the patient has been assigned to. When a patient is referred to UTH, she is assigned to a particular “firm” within UTH.
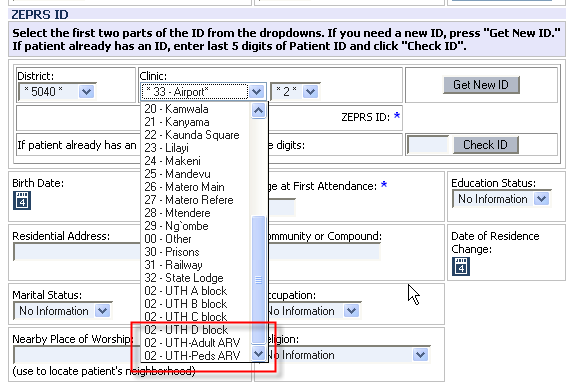
Added Adult ARV and pediatric ARV to patient ID site selection.
Pregnancy Dating
Updates to how LMP/EGA are calculated. This was changed to address a bug: EGA was being calculated by the value for the current date, not by the value entered for “Date of Visit.” In cases where the form was entered after the patient visit, this “Date of Visit” value was not the current date; the calculation of EGA needed to be changed to resolve this bug.
Safe Motherhood: Expansion of the Safe Motherhood care section shows the importance of HIV care in Lusaka.
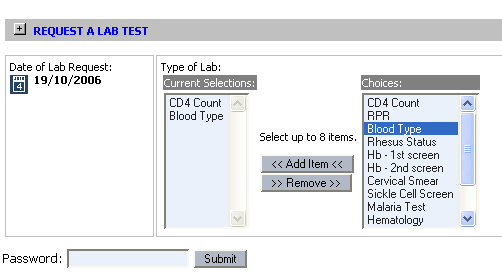
Labs – Clinicians indicated that the process of adding Lab requests took too long because only one Lab request could be made at a time. We changed the way this section works: A user may now make multiple lab requests, which subsequently appear in the problem list displayed on every page. When the results are ready, the clinician clicks the item from the problem list and enters the results.
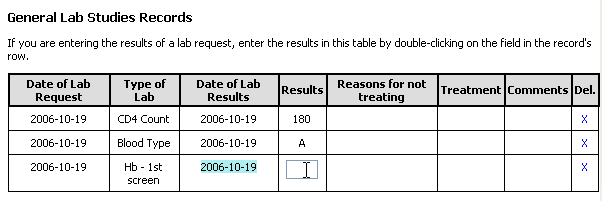
Results of most of the Safe Motherhood-related forms (Labs, RPR, Counsel, etc) are presented in a table to enable easy scanning of lab history.
RPR - For RPR, auto fill Date of RPR screen to today's date (like the HIV test).
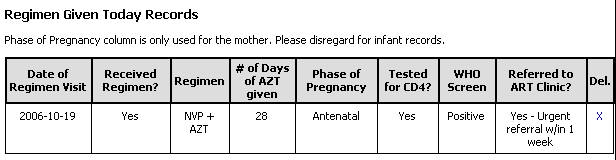
ARV Regimen – added new fields to accommodate the screening with CD4 and WHO staging for severe HIV disease requiring ART and referral to the ART clinic
Hematology – new form
Chemistry – new form
Liver function – new form
Urinalysis – new form
Delivery Summary
Added “Birth Weight” to add newborn widget in order to encourage increased input of this data item.
Reports
Safe Motherhood Register
added new fields
enabled display of column headers on each printed page. Clinics print out this report almost daily and needed the column headers. The “print-only” version includes only recent patients in order to reduce the number of pages printed.
Delivery Register
Added new fields
VCT/ PMTCT Register
Added new fields
Partograph
Extended duration of Partograph based on feedback from UTH – now tracks 24 hours. The previous version did not allow enough hours in cases of long labor duration.
UTH now has capability to re-generate cervix decent plot. Sometimes patients are referred to the UTH from clinics. UTH now has the option to generate new action lines again from where they start treating the patient.
Improved time-tracking capabilities: system now displays actual times rather than hour 1, 2, 3, etc. These times are automatically created based on the time of the first data point entered. Clinicians recommended we make this change in order to keep nurses on-track with their recording and ensure accurate and honest data entry.
Flow changes
After submitting a new Lab, it now returns user to Labs page in case user wishes to submit more Lab requests. This was subsequently changed to enable submission of multiple Labs.
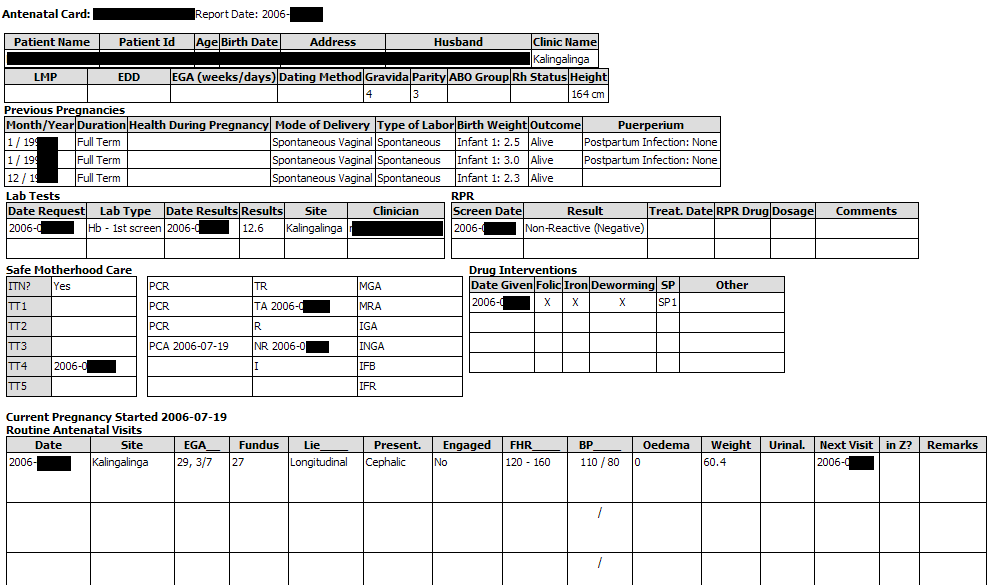
Printed Records
Printable summaries of the patient’s Antenatal record were made available. This summary includes information about routine antenatal visits, coded HIV status (called the HIV Stamp), and medicine info.
Also the printable summary of the Pregnancy after delivery and upon discharge from the hospital– (Pregnancy Discharge Summary)
Form rendering
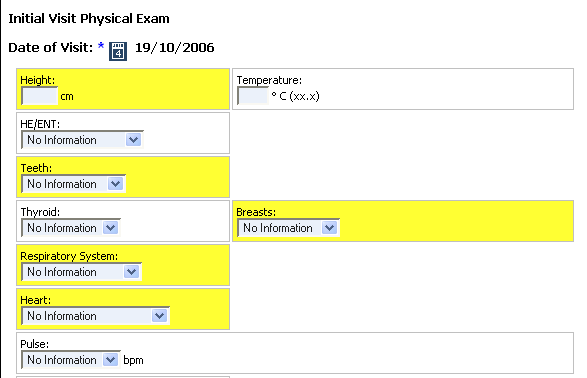
Added capability to highlight particular fields to help user to find the most important fields. Some of the forms have many fields, and clinicians needed a way to easily identify the most commonly used fields. This new capability is currently used in the Initial Visit Physical Exam form.
Offline mode capability – see section below
Administration
Support for Offline Mode.
ZEPRS was originally written to support only a traditional client-server mode - web browser clients interact w/ a single server to submit/view forms, records, and reports. Due to the fact that some clinics were having difficulty maintaining a consistent network connection we needed to look at ways these clinics could continue to use the system during such outages. In response to this need we have enabled ZEPRS to support a disconnected mode, called clinic mode, in which a pc in the clinic can be configured to act as the local clinic server and periodically upload patient records to the main ZEPRS server. This capability is useful in circumstances where network connectivity is unreliable or impossible.
An instance of the ZEPRS application is installed on one of the clinic pc's, which is an ordinary pc except for the addition of 512 MB RAM, making a total of 1GB or RAM. All of the other pc’s in the clinic use the local instance of the ZEPRS application rather than the Master version; therefore, when the site loses connectivity to the Master ZEPRS server, the users at the clinics do not notice this loss.
This clinic "server" is configured to publish an xml file, called an RSS feed, every 30 minutes. The Master ZEPRS server subscribes to this clinic feed. In the same manner, the clinic pc subscribes to the main ZEPRS server RSS feed. The RSS feed is a listing of all of the clinic’s patient records in XML format, with modification dates. When the clinic pc (or master server) imports an RSS feed, it compares each record's last modified date with its own patient records. If the dates are not equal, it downloads an XML file that contains the patient record and updates the necessary data.
More information about Offline mode is available at:
http://rtidemo.org/drupal/node/46
Screen shots of the application in development are provided in the exhibits below. In addition, Flash1 videos of some sections of the application are available at http://rtidemo.org/drupal/node/29
The following exhibit shows the system’s capability to track the UTH Firm to which the patient has been assigned.
The addition of ARV clinic tracking fields reinforces the importance of ARV care.
A lab must be requested before any data may be entered. The following screenshots show how multiple Labs may be requested.
The system creates “Missing Lab Results” notification in the Active Problems section:
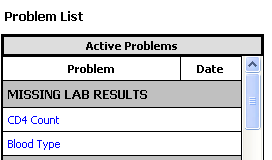
Clicking on the link takes the clinician to the page associated with the request, whereupon she may enter the results.
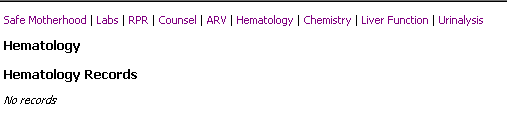
Lab Results may be accessed from links at the top of the Safe Motherhood section.

Exhibit 3: ARV care (Regimen given Today form)
Exhibit 3 shows the addition of more fields to accurately track ARV care.
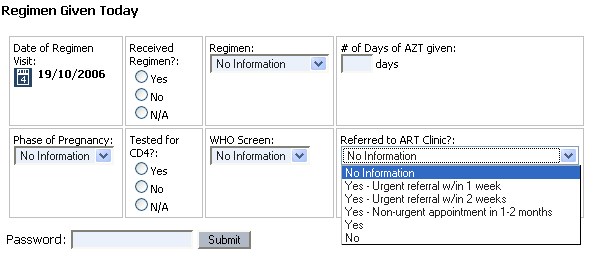
Exhibit 4: Lab Results display
Lab and drug dispensation records are presented in a table that can also be used for data entry..
Display of ARV Regimen Records:
It was noted earlier in this document that results are accessible from links at the top of the Safe Motherhood section pages. The system indicates if no records are available.
Estimated gestational age can be evaluated and reported.
Addition of “Weight” field to Newborn widget was added to encourage data entry of birth weight. It was previously entered only in the Newborn Summary form.

System now presets the timing based on the time of first data entry.
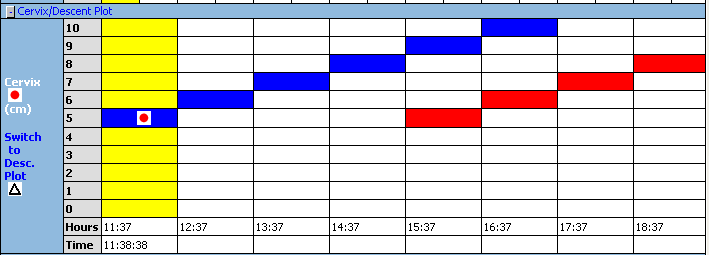
Exhibit 8: Antenatal Monthly Summary Report
This report has been refactored to help with quality assurance (QA) with the missing ANC forms column.
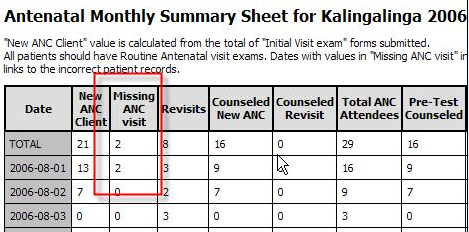
Clicking on one of the “Missing ANC visit” fields provides links to the associated patient records:
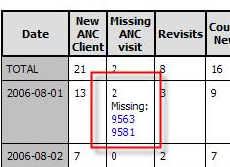
The following fields are now tracked in this report: Date, New ANC Client, Missing ANC Forms, Revisits, Counseled New ANC, Counseled Revisit, Pre-Test Counseled, HIV Tested New ANC, HIV Tested Revisit, Total Tested, Refused Testing, Received Results, Uncollect. Results, HIV Positive:, HIV Negative, HIV Indeterm., Referred ARV Clinic, Maternal NVP, Maternal AZT, Infant NVP, RPR Tested, RPR Positive, RPR Negative, Syphilis Treated, Hgb done, Hgb < 10, SP1, SP2, SP3, TT1, TT2, TT3, TT4, TT5, TT Protected, TT Complete, First visit 1st Trim, First visit 2nd Trim, First visit 3rd Trim, Vermox.
More information about ZEPRS Reports may be found in the ZEPRS Documentation site at the following URL: http://rtidemo.org/drupal/node/37
Clinicians now always print out a summary of the patient’s antenatal visits with each patient visit.
A larger version of this image is available at http://rtidemo.org/drupal/node/50
Exhibit 10: Form rendering enhancement: Highlighting
The following examples show new field highlighting capabilities used to direct attention to commonly used fields. Not so much commonly used but instead it was meant to highlight what should be routinely documented (largely based on existing written documents but also based on medical importance). The goals were to make documentation more uniform and efficient.
During the ZEPRS deployment, CIDRZ experienced problems with equipment and staffing shortages that had a negative impact upon network reliability. Some of the clinics experienced poor connectivity to the ZEPRS network during Q1 and Q2 2006 that inhibited their ability to use the ZEPRS application. Chris Kelley implemented an offline mode system, described earlier in this document, to enable two of the clinics (Kalingalinga and Matero Ref) to use the ZEPRS application while disconnected to the network. Now that network connectivity is improving in Q3 2006, ZEPRS is considering moving these two sites back to normal online operations in order to simplify technical management. The offline mode capability provided the necessary support while it was needed, but would need further development to deploy across the whole ZEPRS network. The offline mode software installation needs to be made simpler, the software used to manage the offline sites could use some improvement, and the clinic wireless installations may need a re-design to permit independent operation while disconnected from the network. Chris Kelley created a “proof-of-concept” standalone client called “Zephyr” that could be used to simplify installation of offline mode clients. More information on Zephyr: http://rtidemo.org/drupal/node/85
Using ZEPRS for direct entry of patient data is successful; nurses are able to conduct their usual patient examinations and perform the necessary data entry into ZEPRS at the same time. This approach is called “Data-entry first.” Dr. Perry Killam meets with clinicians on a weekly basis to identify any issues with the application. Most of the change requests have been of a technical rather than functional nature: to fix bugs in the application or to make minor changes to form fields.
Dr. Killam did identify a couple of changes that needed to be made in order to practically accommodate the “data entry first” approach into the work process. First, antenatal records are now printed at each patient visit only at UTH. At the clinics, they only print the antenatal card during the first visit then both write on the card and update ZEPRS. This process is counter to the original intentions of ZEPRS: to eschew any printing of records by clinicians due to the high cost for printer paper at the inception of the project. This goal proved to be unrealistic, especially while ZEPRS is not deployed across all Lusaka clinics. Patients needed a record of antenatal care when visiting non-ZEPRS clinics. Adding this printout capability provided the necessary remedy. The second change was in regards to the partograph. Nurses on midnight duty must accommodate a heavy patient load; they were having real difficulties entering data on 20 deliveries at the same time. At the moment they are entering on paper first and then entering in to the ZEPRS system as time permits. CIDRZ has created a new paper form, based on two ZEPRS forms. This new paper form features Labor Admission on front and the Partograph on the back for this new process.
CIDRZ has been working with the CDC since November, 2005 on a patient tracking system for anti-retroviral therapy. This system has been mandated by the Zambian government to become the official ARV care system for the whole country. This system is now planning to include support for perinatal care and will ultimately replace the ZEPRS application. Dr. Killam and Mr. Kelley will work with the CDC’s software engineers to duplicate the ZEPRS application functionality into this new application. This new system is expected to be deployed mid-2007.
1 Flash is a registered trademark of Macromedia, Inc.
RTI
International Page